For any pregnancy to occur, natural or assisted, an egg must be fertilised by a sperm. This would normally happen in a woman’s fallopian tubes in the few days after sexual intercourse when large amounts of sperm are present in her reproductive tract. However, when a woman or couple undergo in vitro fertilisation (IVF), the egg and sperm are brought together outside the body. In this article, we look at the different ways embryologists can bring egg and sperm together in the lab and how we know when fertilisation has and hasn’t been successful.
The steps involved in fertilisation
1. Egg stimulation and maturation
During your natural cycle each month, the ovaries release a single, mature egg. When you have IVF, your fertility specialist will prescribe hormone medications to help several of your eggs mature at once. This increases the number of eggs available for collection at the time of egg retrieval.
How do we know if your eggs are mature?
An egg is made up of an outer shell called the zona pellucida, which forms a protective case around the egg to protect the internal structures and assist with fertilisation. If you have ever studied biology at school, these internal structures include the cytoplasm, organelles and DNA.
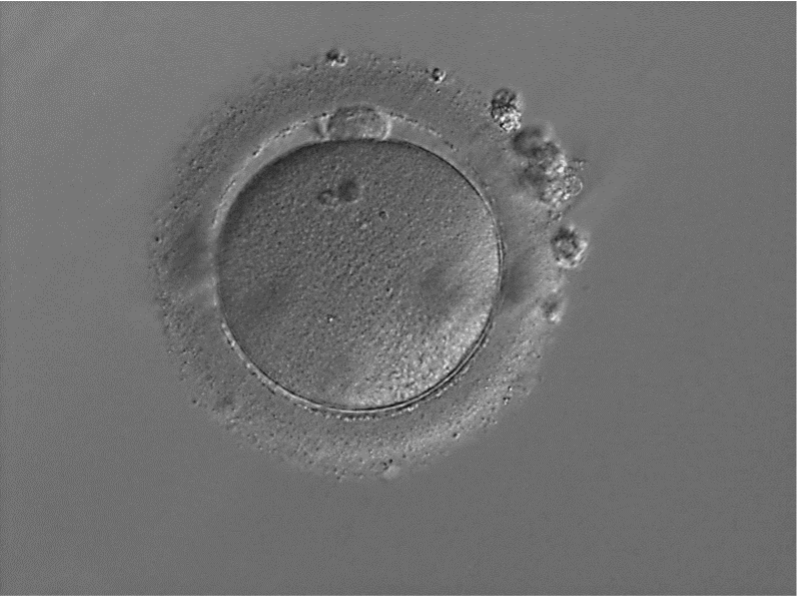
Eggs are classified as mature when a small cell (called the polar body) has been released and is visible within the shell of the egg (Figure 1).
Figure 1 – A mature egg has a small cell sitting on top of the egg known as a polar body; in this photo, the polar body can be seen at about 12 o’clock
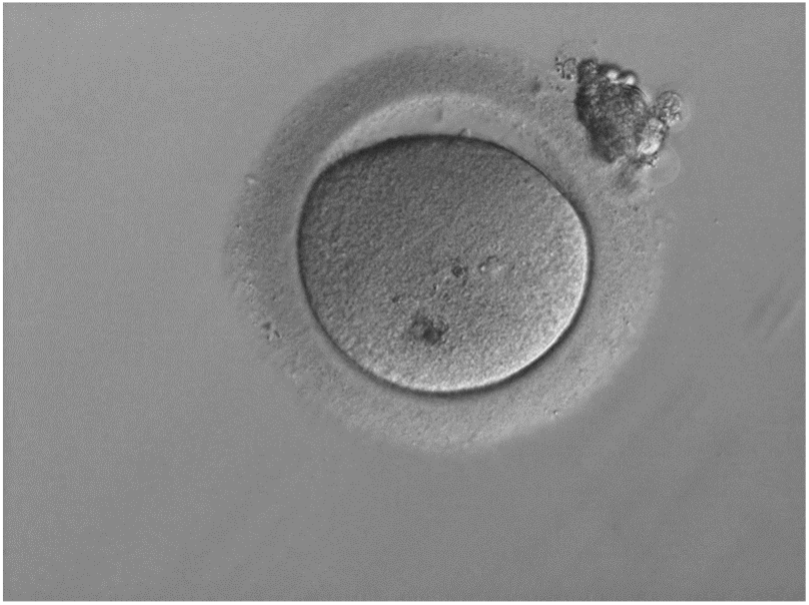
Sometimes, despite giving you hormone medication during the stimulation phase of IVF, your eggs remain immature. This occurs when maturation has started but hasn’t fully completed in time (Figure 2). These eggs may mature with time; however, when inseminated they may not fertilise at a high percentage. Unfortunately, if they don’t mature, these eggs cannot be used in the next stage of IVF (insemination).
Figure 2 – An immature egg in Metaphase I (MI) stage does not have a polar body as it has not yet been released and is not suitable for insemination
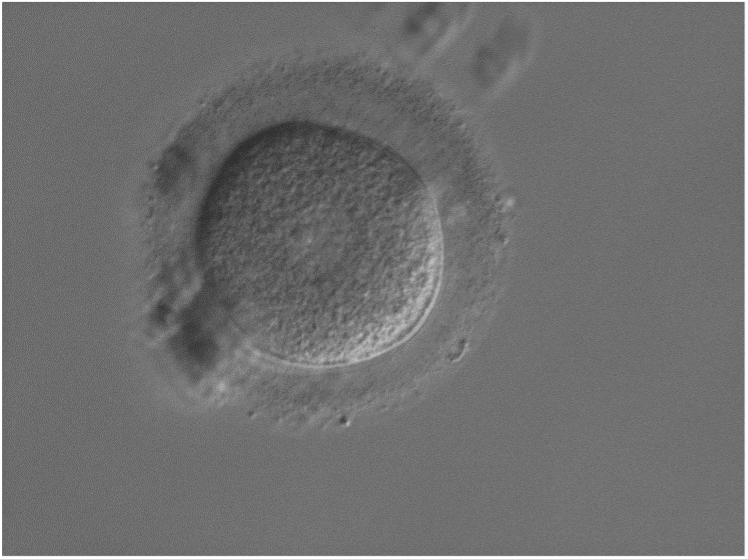
Very immature eggs (stuck at what we call the germinal vesicle stage) are distinguished by a larger, central circular nucleus (Figure 3). These eggs will not be able to fertilise and so they also can’t be used in the next stage of IVF (insemination).
Figure 3 – Very immature eggs have a circular structure in the middle called a germinal vesicle and will not fertilise
2. Insemination (bringing sperm and egg together)
In the IVF lab, there are two different methods we can use to bring your egg and sperm together:
Conventional IVF (natural insemination)
During conventional IVF, we let egg and sperm come together naturally by placing around 100,000 sperm in a special laboratory dish with 1–2 eggs we have collected and its supporting cells. Once a sperm has penetrated the egg’s supporting cells, it gains entry to the egg by sticking to, then penetrating the egg’s outer shell. In order for this to occur, both the egg and the sperm need to be mature. Mature sperm have specialised structures that allow them to successfully gain entry to an egg. While a 100,000 sperm will be placed with your egg, unfortunately, this still does not guarantee that one pair will successfully come together and fertilise.
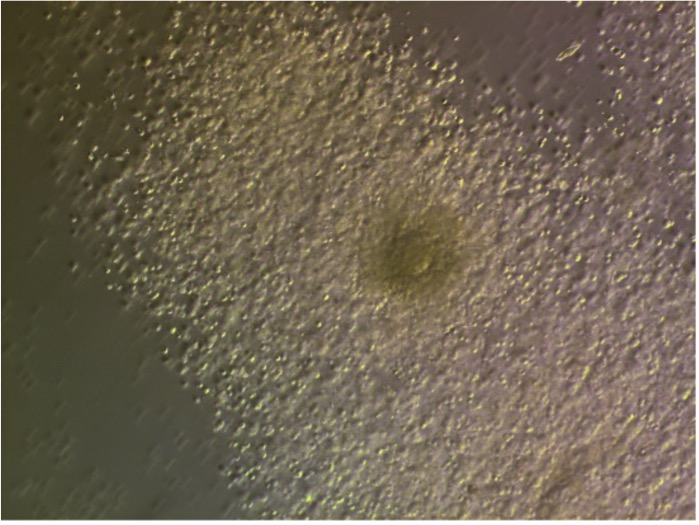
Figure 4 – An egg (the dark circular structure in the middle) with its supporting cells surrounding it (called the cumulus-oocyte complex) at the time of egg retrieval
IVF + ICSI (assisted insemination)
Sometimes during IVF we will give fertilisation an extra helping hand by using a special procedure called ICSI, instead of leaving egg and sperm to come together in a lab dish. Typically we will use ICSI when there are issues with the male partner’s sperm that preclude natural insemination in a lab dish or when conventional IVF has been attempted and was unsuccessful. ICSI stands for IntraCytoplasmic Sperm Injection and involves very precisely injecting a single, healthy sperm into a single, mature egg.
During ICSI, we first remove the supporting cells around your egg to determine if it is mature. This also helps us visualise the egg, so we can see where its DNA is. We can then position the egg appropriately so that when we introduce the sperm, we do not disrupt the DNA. Before we do this, we must also ensure that the egg’s membrane has been successfully penetrated, so that we can deposit sperm inside your egg.
When we inject a sperm into an egg, we apply gentle pressure with a special pipette (called an injection pipette), which has been pre-loaded with the sperm. Sometimes, an egg’s membrane has a lot of resistance and other times there is little or no resistance. Every now and then, the membrane of an egg may give way to the pressure of the injection pipette and break apart. If this occurs, we can no longer use this particular egg.
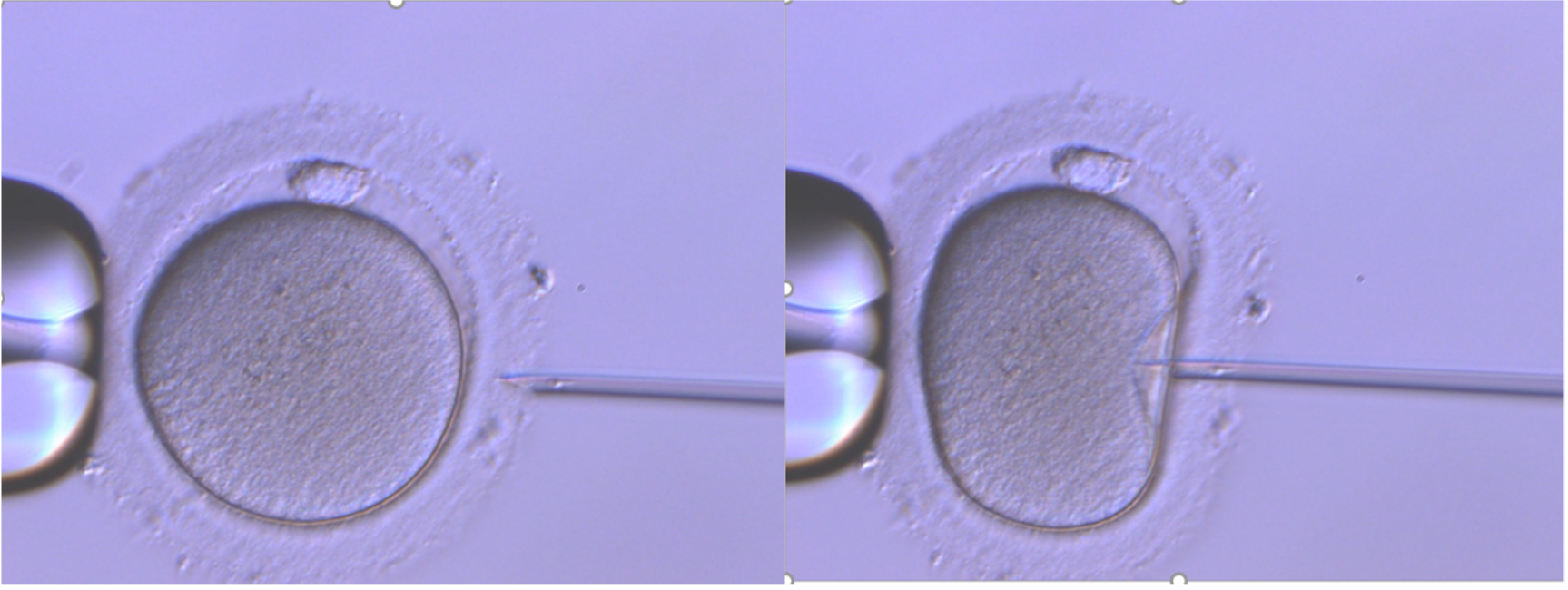
Figure 5 – A mature egg undergoing ICSI: the left image shows the holding pipette while the right image shows the injection pipette loaded with sperm
The outcomes of insemination
Normal fertilisation
Following insemination, we can tell if a sperm has successfully fertilised an egg by looking for special structures inside the egg. In the case of normal fertilisation, we will see two distinct circles inside the egg called the pronuclei – these contain DNA from the sperm and egg (commonly referred to as 2PN, meaning two pronuclei). A second little cell (another polar body) is also released from the egg under the zona pellucida (eggshell). This can be seen the morning after insemination (day 1).
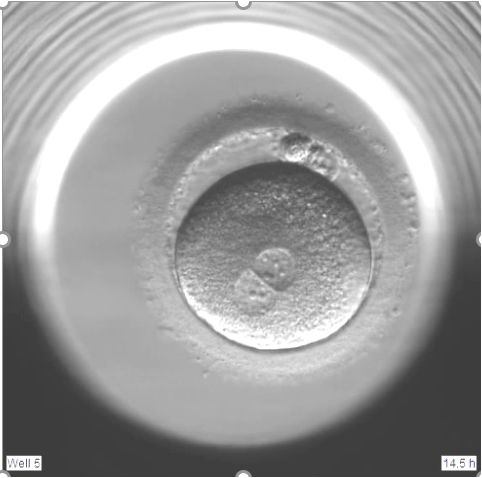
Figure 6 – Two polar bodies (about 1 o’clock) and two pronuclei (about 7 o’clock) are present, indicating that the sperm has successfully fertilised the egg
Atypical fertilisation
When an inseminated egg displays more or less than 2PN, then we classify this as atypical fertilisation.
1PN
Figure 7 – A 1PN embryo, or monopronuclear embryo, is a fertilised egg that has one pronucleus instead of two.
A 1PN is a fertilised egg that appears to have only one pronucleus. This occurs in approximately 3–5% of inseminated eggs. An inseminated egg that displays 1PN is classified as atypical.
Several factors can lead to the formation of a 1PN fertilised egg, including:
Early fusion of genetic material – The egg and sperm’s DNA may be close together, resulting in a single pronucleus surrounding both sets of DNA
Egg activation without sperm (parthenogenesis) – The egg may start developing without fertilisation. Therefore, only the egg’s DNA is present
Fertilisation with only sperm DNA – Only the sperm’s genetic material participates in fertilisation. The egg’s genetic material is not contributing, therefore preventing normal development.
These atypically fertilised embryos are less likely to develop to the blastocyst stage. However, if they progress to the blastocyst stage, genetic testing helps us determine if they have both maternal (egg) and paternal (sperm) chromosomes. Further, we can determine if these embryos can be considered for (embryo transfer).
3PN+ embryo
Figure 8 – A 3PN embryo is a fertilised egg that has three pronuclei.
In around 1–5% of inseminations, three or more pronuclei may be visible. An inseminated egg that displays 3PN or more is classified as atypical.
Several factors can lead to the formation of a 3PN fertilised egg, including:
The inability of the egg to block polyspermy: During conventional IVF, the egg’s natural defence against multiple sperm entry is not effective, allowing more than one sperm to enter the egg. This results in more than 1 set of paternal (sperm) chromosomes to be present
Abnormal egg activation: Premature/improper activation of the egg; or the second PB of the egg is not released, which can result in 2 sets of maternal (egg) chromosomes present
Sperm quality issues: Abnormal sperm may increase polyspermy risk (see point 1).
There is a high chance that these embryos are genetically abnormal and extensive genetic testing is required before considering these embryos for transfer.
With the advances in genetic testing capabilities, we can perform ‘molecular fertilisation assessments’ on embryos that have displayed atypical fertilisation and reach the blastocyst stage. This means that, with the appropriate testing, we can potentially increase the number of embryos for transfer. Embryos that do not show signs of the second polar body being released (and therefore the second set of maternal chromosomes released) would not be considered for testing as these embryos are considered abnormally fertilised.
If you are interested in testing your atypically fertilised embryos that reach the blastocyst stage please discuss this with your fertility specialist or a Newlife IVF staff member before commencing treatment. We will let you know if you have embryos that fall into this category and update you if they are developing. Please be aware there are fees involved in testing these embryos and these are per embryo and dependent on the type of testing required.
Non-fertilisation
Fertilisation is a complex process requiring precise interactions between the egg and sperm. There are several reasons why eggs may not fertilise, including:
Sperm-related functioning: Even with ICSI, some sperm may not provide the necessary signals for egg activation
Egg quality: Eggs may lack the ability to respond to a sperm’s activation signals
Lack of calcium oscillation: During normal fertilisation, sperm triggers calcium waves in the egg that initiate fertilisation and embryo development. In some cases, this process doesn’t occur as expected
Unexplained factors: Despite no obvious abnormalities, fertilisation may still not occur.
If no pronuclei are present and a second polar body has not been released, the egg has not been successfully fertilised. Alternatively, if no pronuclei are present and the second polar body has been released, this indicates that fertilisation started but did not reach completion. Once the sperm enters the egg, several reactions must occur for the fertilisation process to be successful. If components are missing from the egg or sperm or interactions are unable to occur, fertilisation will not be achieved.
Immature eggs
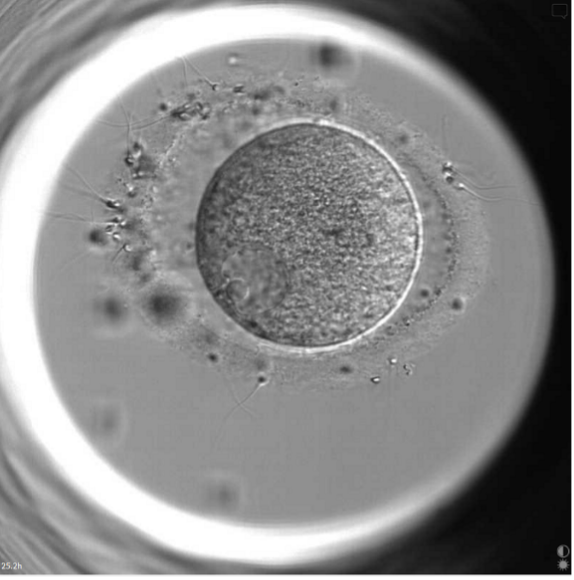
Figure 9 – An egg at the very immature germinal vesicle stage: sperm have tried to fertilise this egg (as seen by the sperm attaching to the outer shell of the egg), but because the egg is immature, sperm cannot fertilise the egg.
Unfortunately, these eggs will not form viable embryos and cannot be used in the next stage of IVF (embryo transfer).
Understanding the outcomes of fertilisation and insemination during your IVF cycle
While many different factors influence whether fertilisation during IVF is successful, having healthy, mature eggs and sperm are most critical to success. We understand every egg is precious, and we will give every egg the chance to be a viable embryo.
If you have questions at any time during your cycle, you can call (03) 8080 8933 to speak to our patient support team. They will direct you to your Newlife IVF fertility specialist, fertility nurse, fertility counsellor and/or embryologist as appropriate for the information and support you need.
Image credits: all photos shown are from the Newlife IVF laboratory.
The information on this page is general in nature. All medical and surgical procedures have potential benefits and risks. Consult your healthcare professional for medical advice specific to you.