I’m a single woman – what are my options?
Donor sperm – clinic-recruited versus known donors
Essentially, there are two options for obtaining sperm: accessing donor sperm through a fertility clinic’s sperm bank, or using a sample provided by someone you know.
At Newlife IVF we have an on-site sperm bank containing samples recruited from local and international donors. The benefit of using sperm from our clinic-recruited donors is that it is thoroughly tested for infectious diseases and common genetic problems. After we freeze the sperm, it is then quarantined before donors are retested to make sure it is high quality and safe to use.
When you use a clinic-recruited donor, you also have the advantage of very clear legal boundaries. The donor has no legal connection to your child – they are not entitled to custody and do not have to pay child support. They also remain anonymous to a large extent; that is, you will not know the donor’s identity (but you will know their family medical history and some of their traits). However, your child can request that the donor’s identity be revealed to them when they turn 18.
If you choose not to go the clinic-recruited donor route, you may consider using a sperm sample from a friend or acquaintance. A benefit of using a known donor is you will likely have a good understanding of their appearance, background and traits. However, the social and legal boundaries are not as clear-cut as they are when using a clinic-recruited donor. Discussing expectations and creating firm boundaries with a known donor requires careful negotiation, and you may wish to seek legal advice on how best to proceed.
If you do decide to use a sample from someone you know, it’s best to involve a fertility clinic. That way, you can have the sample rigorously tested for safety and quality in the same way we test donor sperm.
In this video, Dr Chris Russell talks about donor sperm and its use in IVF and IUI procedures.
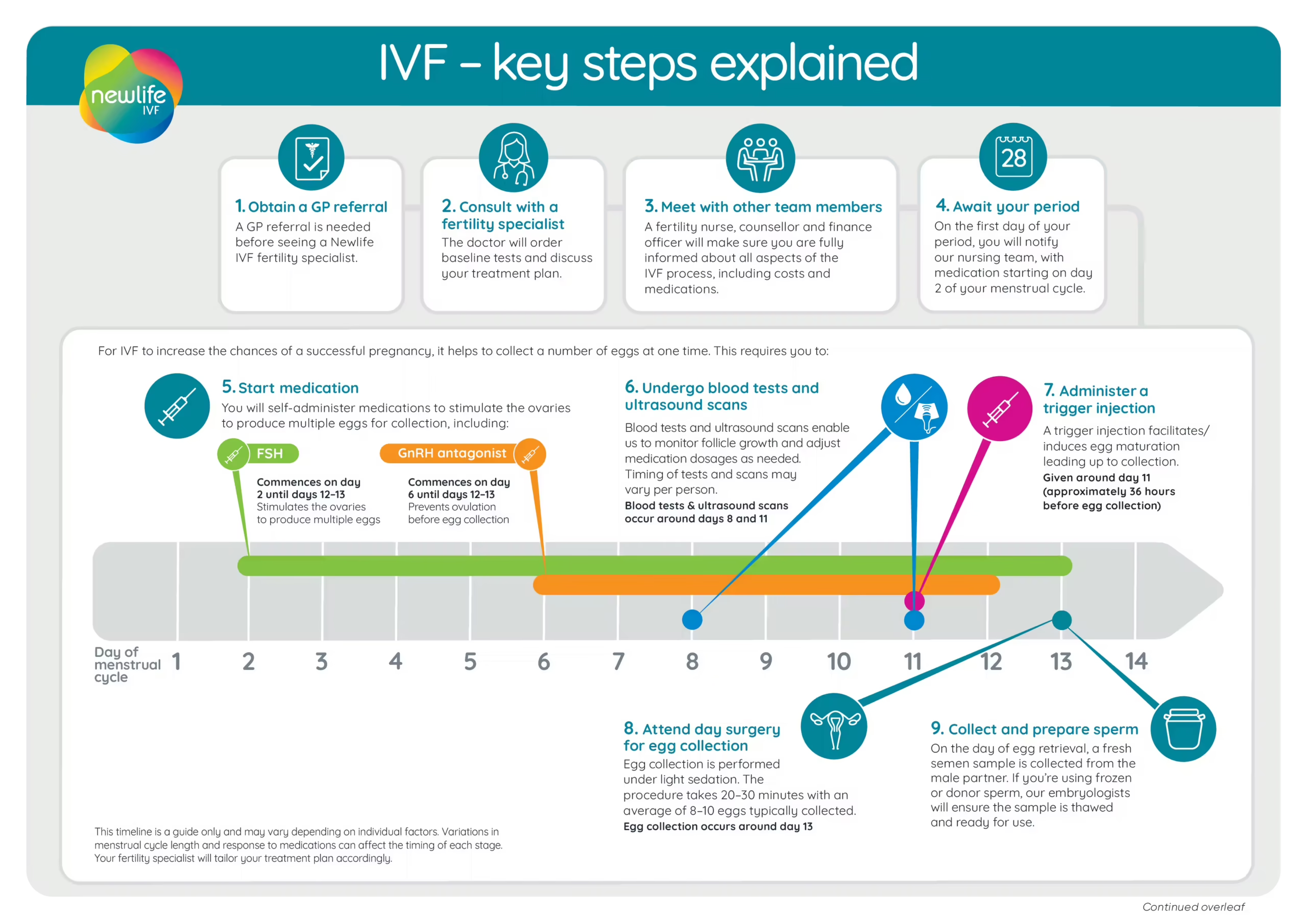
Insemination – how egg and sperm meet
The next consideration is how best to introduce the sperm sample to your egg. There are a few different options for insemination, and the most suitable will depend on your specific circumstances.
One possibility is home insemination. In this method, sperm is injected into the vagina using a syringe at home. As this mimics the natural fertilisation process, home insemination is effective when the donor has a normal sperm count. It is also one of the most cost-effective options. However, it does not afford the same degree of protection from infectious disease as undergoing a similar process via a fertility clinic.
The clinic-based alternative is intrauterine insemination (IUI). This is where a sperm sample is concentrated to contain a very high number of sperm. It is then injected directly into your uterus soon after your ovaries release an egg. Using a concentrated sperm sample increases the chances of a sperm fertilising your egg. Depending on your circumstances, your specialist may recommend combining IUI with a medication to stimulate the release of an egg from your ovaries, further increasing the chance of success.
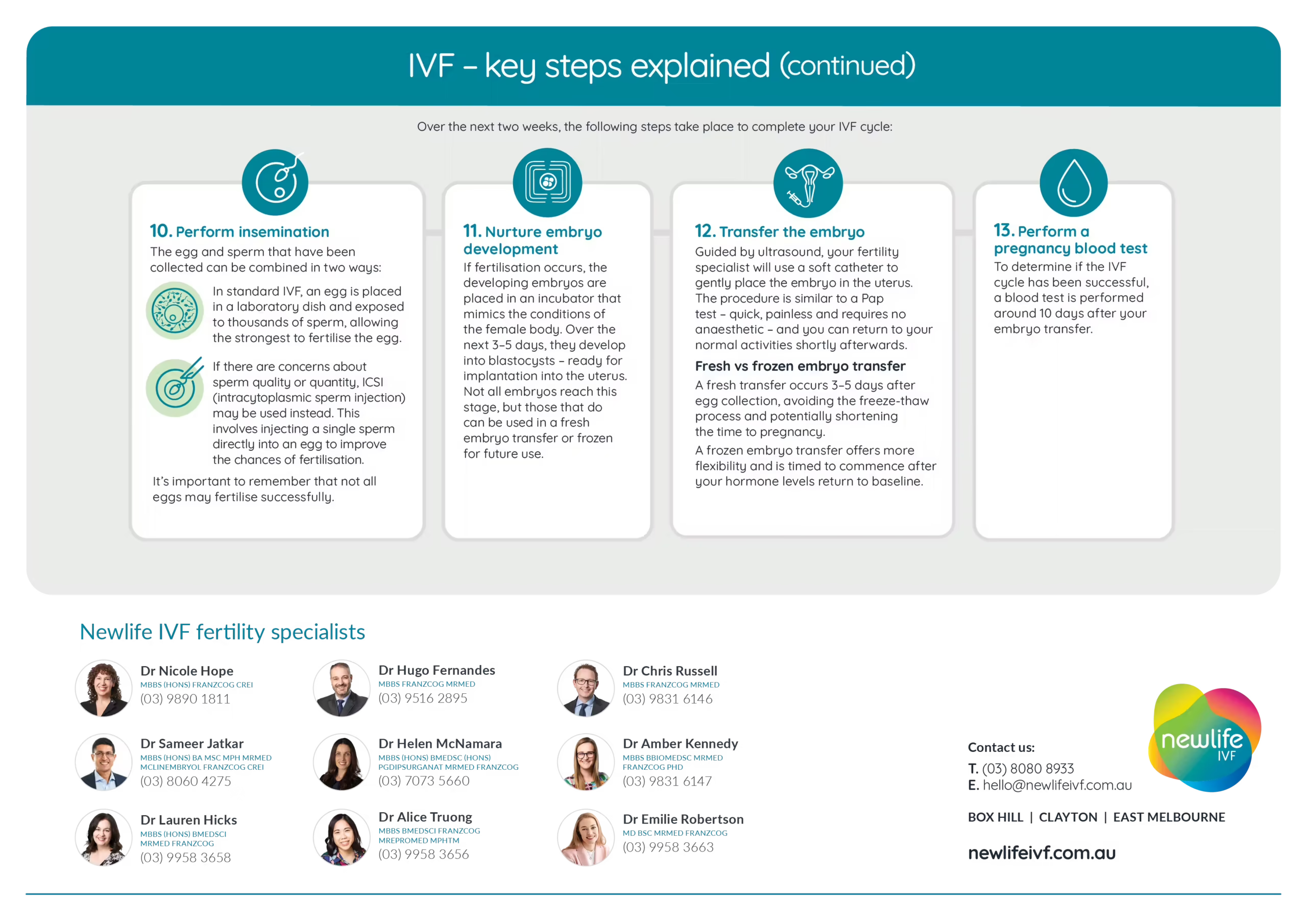
The last option is in vitro fertilisation (IVF). In this process, several of your eggs will be introduced to sperm in laboratory dishes. When utilising clinic-recruited donor sperm, the best sperm may be selected and a single sperm injected directly into each egg, a process called intracytoplasmic sperm injection (ICSI). One of the best embryos resulting from IVF insemination will then be transferred back to your uterus. The rest can be frozen and stored for later use, if necessary.
There are a few reasons you may be advised to undergo IVF. If you have known infertility, you’re in your late 30s or early 40s (when female fertility naturally declines significantly), or you struggle to get pregnant through other forms of insemination, your specialist may recommend this procedure. Likewise, IVF may be advisable if you’re using a known sperm donor with low sperm quality or quantity for other methods of insemination. If you wish to do preimplantation genetic testing, which is the process of genetically testing your embryos before they are transferred to your uterus, IVF will be necessary. For more information about these procedures in relation to your particular circumstances, chat to your fertility specialist.
I’m a single man – what are my options?
To have a baby as a single man, you will need the help of an egg donor and a surrogate. According to Victorian law, these must be two different women.
You may choose to use a clinic-recruited egg donor, or a known donor, i.e. a friend, acquaintance, or a family member (note: the last is only okay if you are not using your own sperm). Egg donation must be altruistic in Australia, meaning no financial compensation is paid for providing eggs. Once the donor eggs are ready, your sperm will be introduced to them using IVF (discussed earlier in this article), and the best resulting embryo will be transferred to your surrogate’s uterus. If you are not using your own sperm, donor embryos may be an appropriate option for you.
It’s common to ask a friend, acquaintance or family member to be a surrogate. Surrogacy is also an altruistic process in Australia, however ‘reasonable’ medical costs can be paid by you. Keep in mind that in Victoria, multiple medical consultations, counselling sessions and legal advice are required for both you and the surrogate prior to proceeding. You will also need to seek permission from the Patient Review Panel (this is a legal requirement in Victoria), and the sperm or embryos must be quarantined. This process can take several months.
Seeking a surrogate overseas may also be an option. However, according to Australian law, this is only legal if it is altruistic. Be aware that this is a very expensive route and you will need to plan to potentially be overseas for a few months after your baby is born to organise their entry into Australia.
For advice related to your particular circumstances, you may wish to seek legal advice and talk to a fertility specialist. Unfortunately, Newlife IVF is not permitted to assist you in finding a surrogate (nor can any other IVF provider). However, our counsellors can certainly orientate you to the Victorian surrogacy community and provide support and information as you look for a potential surrogate.
Ready to have a baby on your own?
Make an appointment with one of our caring and experienced Newlife IVF fertility specialists to discuss the most appropriate way forward based on your medical history, circumstances and preferences. Call (03) 8080 8933 or book online and take the next step towards your dream.