After retrieval, the egg and sperm are combined, and if fertilisation is successful, your embryo spends the first few days growing in the lab under the expert care of our team. This blog will help guide you through these early embryo development steps before transfer or freezing.
Factors affecting embryo development
Embryo development is a complex process that requires a combination of genetic, environmental and physiological factors to progress successfully. To achieve good embryo development, we require:
Healthy egg and sperm
The egg and sperm provide the genetic blueprint for development. Each embryo needs a complete set of 46 chromosomes – 23 from the egg and 23 from the sperm. Some embryos inherit incorrect genetic instructions that can impact embryo development and make it harder for them to divide and grow as expected.
Mitochondrial energy
Embryos need energy to divide and grow, which is provided by mitochondria (tiny energy-producing structures in cells). Poor mitochondrial function can slow or stop embryo development.
Efficient metabolic function:
An embryo’s metabolic function provides both energy and the building blocks needed for development. This includes the creation of protein and fats, and the removal of waste products that can be toxic to the embryo. Together, these provide what the embryo needs for growth, cell division and viability.
Timely cell division
Embryos should ideally divide at a regular pace (2-cell, 4-cell, 8-cell, etc.). Uneven and/or delayed division can mean the embryo is of suboptimal quality and may not develop as expected.
Embryonic genome activation
Around Day 3 (see diagram below), embryos start using their own DNA instead of relying on maternal DNA (genetic code from the egg). If this DNA transfer is inadequate, interrupted or missing, this can slow or stop the development of an embryo.
Stable conditions
Embryos need the right temperature, oxygen and pH balance to grow. These factors are carefully assessed and monitored continuously in the laboratory environment.
Difficulties or inaccuracies in any of these processes can affect the way an embryo grows and can impact whether an embryo will reach the blastocyst stage (where it has divided into many cells), making it suitable for transfer or freezing.
Safeguarding your embryos is our highest priority
We understand how important every embryo is to your journey. That’s why we use the most advanced technology and scientifically proven methods to create the ideal environment for embryo development. From carefully performing every procedure to closely monitoring each embryo’s progress, our highly trained embryologists work tirelessly to give each embryo the best possible chance to grow and thrive.
We maintain strict laboratory conditions, including precise temperature, humidity and air quality control to mimic the natural environment as closely as possible. Our team carefully observes each embryo’s development at every stage. Even though not all embryos will reach the blastocyst stage, please know that we do everything in our power to maximise their potential. Your dream of building a family is at the heart of everything we do, and we are committed to providing the best possible care every step of the way.
If you have any questions about embryo development or your fertility journey, please reach out to Newlife IVF. In the meantime, let’s walk through the different stages of embryo development to help you better understand the process.
For fresh embryo transfers, all embryos are assessed on the morning of day 5, and we select the embryo that is progressing the best at that time. For frozen embryo transfers (FETs), embryos are reviewed and selected the day before the transfer. Information on how we track embryos can be found here.
How do we select embryos for transfer?
Selecting an embryo for transfer, when there is a cohort of embryos to select from, can be a complex process that involves assessing multiple factors, including utilisation of advanced technology. Here’s how we carefully evaluate embryos to choose the embryo for transfer from a cohort:
1. Genetic testing (if performed)
If your embryos have undergone genetic testing, known as Preimplantation Genetic Testing (PGT), the genetic results are weighted above all other embryo selection methods. Embryos with the correct number of chromosomes are considered suitable for transfer, which helps to reduce the risk of miscarriage or genetic conditions related to chromosome issues. This testing allows us to focus on embryos with the best chance of resulting in a healthy pregnancy. More information on PGT-A results can be found here.
2. Embryo grading system
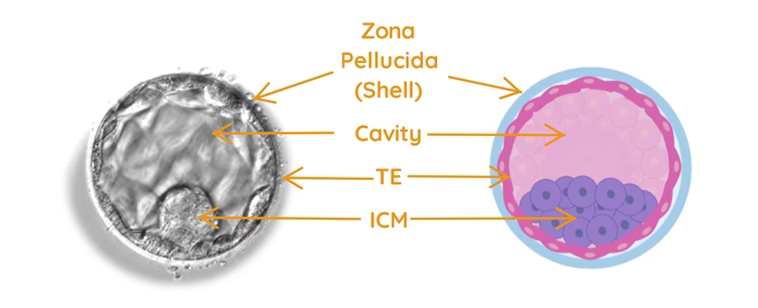
We assess the embryos based on their appearance using our blastocyst grading system. Embryos typically develop to the blastocyst stage around day 5 or 6 of culture. We assess their degree of expansion (i.e. the number of cells), along with the appearance of two key cell groups: the inner cell mass (ICM) and the trophectoderm (TE). Both the ICM and TE are graded from A to D based on their structure and appearance. As there are several factors that are taken into consideration for embryo grading, we also consider timing of the evaluation when we review the embryos for selection. The grades are only indicative of appearance at the time of assessment and this may change with time. Grade A and B embryos are considered good quality in appearance, and Grade C embryos remain viable and capable of resulting in healthy pregnancies. Grade D embryos are considered non-viable and are not suitable for transfer or freezing.
You can find more information on embryo grading here.
3. Monitoring embryo development using time-lapse imaging and artificial intelligence (AI)
We continuously observe and review embryo development over 5-6 days using a special time-lapse imaging system. Embedded Artificial Intelligence (AI) analyses factors such as the appearance of cells, the timing and pattern of cell divisions, and other key developmental events. AI helps prioritise those with the highest potential for implantation and pregnancy. While AI is a valuable support tool, it has limitations; for example, if an embryo has residual support cells attached or excluded cells, AI scoring may be less reliable. Therefore, embryologists use their expertise assessing the videos and the embryos’ morphological milestones alongside AI and the grading system to make the best possible selection.
Integrating all factors to select the best embryo
All these factors (i.e. genetic testing results, embryo grading, AI scores and embryologist expertise) are carefully combined and taken into consideration when selecting embryos. We compare embryos based on this comprehensive information to identify those with the highest potential for successful implantation and pregnancy. However, it is important to understand that every embryo transferred has the potential to form a pregnancy, even those with lower grading or scores, as embryo development and appearance is not always indicative of its developmental potential.
Preparing the embryo for transfer
Selected embryos are chosen either on the morning of day 5 for fresh transfers or the day before for FETs. On the day of transfer, the frozen embryos are carefully thawed and we expect over 97% of embryos to successfully thaw. There are rare instances that an embryo may not survive the freeze/thaw process and in this instance, we will thaw another embryo if available and we will inform you. If there are no other embryos frozen, we will call you to let you know. After warming, the embryos are placed in specialised incubators designed to maintain the ideal environment until the time of transfer.
Enhancing implantation with a quality transfer medium – EmbryoGlue
At Newlife IVF, all embryos are transferred using a medium called EmbryoGlue, which is rich in hyaluronan, a substance found naturally in the uterus. EmbryoGlue is designed to enhance the embryo’s ability to implant into the lining of the uterus. Several studies suggest that EmbryoGlue may improves clinical pregnancy and live birth rates (Heymann et al., 2020; Adeniyi et al., 2021; Tyler et al., 2022; Reed et al., 2022). While these findings are promising, we continuously monitor new research to provide care based on the latest scientific evidence. You can read more on how we give embryo transfer the best chance of success here.
Best scientific practice
At Newlife IVF, we combine all available technology and the expertise of our embryologists to carefully select embryos with the best potential of resulting in a healthy pregnancy. We only transfer embryos that we believe have a chance of success because we know how much every cycle means to you. Please be reassured that even the final embryo remaining has the potential of achieving a pregnancy. If you have any questions about the embryo selection process or your specific treatment, please feel free to discuss them with your Newlife IVF team.
Witnessing in IVF refers to the process of confirming that the correct eggs, sperm and embryos are used for the correct patient at the correct time. It mitigates the risk of mismatched or misidentified samples. At Newlife IVF, we take this responsibility extremely seriously, which is why we use both electronic and manual methods for accuracy and traceability.
RI Witness – electronic tracking for your peace of mind
Newlife IVF employs the RI Witness electronic witnessing system, which uses Radio Frequency Identification (RFID) technology to track and verify all eggs, sperm and embryos in the laboratory. Each patient is assigned an RFID card and every patient vessel (e.g. tubes, dishes and cryo-vessels) is labelled with a matching RFID tag, all of which are programmed with each patient’s unique IVF code and three points of identification.
How RI Witness works at Newlife IVF:
Patient RFID card: you are assigned an RFID card that is linked to your profile. This is used for identification during key procedures, such as egg retrieval and embryo transfer
RFID tags on all labware: all test tubes, dishes and cryo-vessels used to hold your biological material are labelled with RFID tags matched to your unique code and profile
Real-time monitoring: all lab workstations have RI Witness receivers that detect these tags automatically. The system logs and monitors every sample movement during the procedure in real-time
Mismatch protection: if a mismatch ever occurs – for example, if two different tags are brought into an area at the same time – RI Witness triggers an audible and visual alarm, and the procedure is stopped immediately to investigate and correct the issue. To further reduce the risk of mismatches, our embryologists strictly work with the biological materials of only one patient at a time at each workstation.
Cryostorage tracking
All biological material placed into cryostorage is barcoded and tagged using the RI Witness system.
Each cryo-vessel is labelled with:
Your full name
Date of birth
Unique IVF code
Date of freezing
Barcode is specific to the eggs, sperm or embryos stored inside.
These cold-resistant tags ensure identification is maintained even at ultra-low temperatures. When the material is removed from cryostorage, the barcode is scanned and cross-verified with RFID data and RI Witness, and double-witnessed by embryologists to confirm all points of identification.
Embryologist double-witnessing
In addition to RI Witness, every procedure is manually witnessed by two embryologists. This human double-checking system complements electronic witnessing and adds a layer of human judgement, visual verification and accountability.
Manual witnessing includes:
Verifying three patient identifiers (full name, DOB and patient unique IVF code)
Cross-referencing all vessel labels, barcodes and RI Witness tags
Confirming the procedure that is to take place
Checking the freeze dates and, for embryos, specific embryo numbers
Confirming the correct sample before and after thawing.
This step is essential when biological material is entering or exiting the laboratory, and before every procedure such as insemination, embryo transfer, embryo biopsy or cryopreservation.
Cryostorage safety – cryo-vessel monitoring and audits
Biological materials such as eggs, sperm and embryos are stored in specially designed devices (cryo-vessels) that are specific for very cold temperatures. The cryo-vessel is tagged with a special tag that withstands very cold temperatures. The cyro-vessel includes the patient’s name, date of birth, unique IVF code and the date of the freezing, along with a unique barcode that is specific to that patient’s egg, sperm or embryo held within the individual device.
Every sample is:
Uniquely identified and traceable
Matched at any time using the RI Witness system and barcode
Manually verified when moved or thawed.
Regular audits are conducted, comparing all stored material against patient records, to ensure that what is in storage precisely matches what is documented in each individual file and the RI Witness log.
Thawing of stored biological material
When biological material is removed from cryostorage, the barcode is scanned and linked to the patient’s vessel via an RFID tag. Removal of eggs, sperm or embryos from cryostorage is also witnessed manually by the embryologist performing the procedure and a second embryologist. Before thawing the biological material, the embryologists will witness the three points of patient identification on the cryotag, the freeze date and, in the case of embryos, the specific embryo number on the cryotag. This is cross-referenced with the vessel the biological material will go into after thawing, and the RI witness system. A mismatch at any point will sound an alarm.
Only once all of these steps have been completed will the thawing of the eggs, sperm or embryos proceed.
Summary of witnessing measures at Newlife IVF:
Only one patient’s material is handled at each workstation at any time
All vessels and labware are RFID tagged and barcoded
The RI Witness system and the embryologist manual double-witnessing are used to confirm all details at every procedure
Cryostored material is linked to the patient via a barcode and the RI Witness system.
Regular audits verify that frozen material in storage matches patient records and the RI witness system.
Please ask us!
We understand IVF can be a time filled with both hope and uncertainty. Our systems are designed to mitigate risk and ensure your biological material is being managed with the highest levels of care, security and accountability. If you have any questions, please speak to a member of our team. We’re always happy to help you feel supported and informed.
During your natural cycle each month, the ovaries release a single, mature egg. When you have IVF, your fertility specialist will prescribe hormone medications to help several of your eggs mature at once. This increases the number of eggs available for collection at the time of egg retrieval.
How do we know if your eggs are mature?
An egg is made up of an outer shell called the zona pellucida, which forms a protective case around the egg to protect the internal structures and assist with fertilisation. If you have ever studied biology at school, these internal structures include the cytoplasm, organelles and DNA.
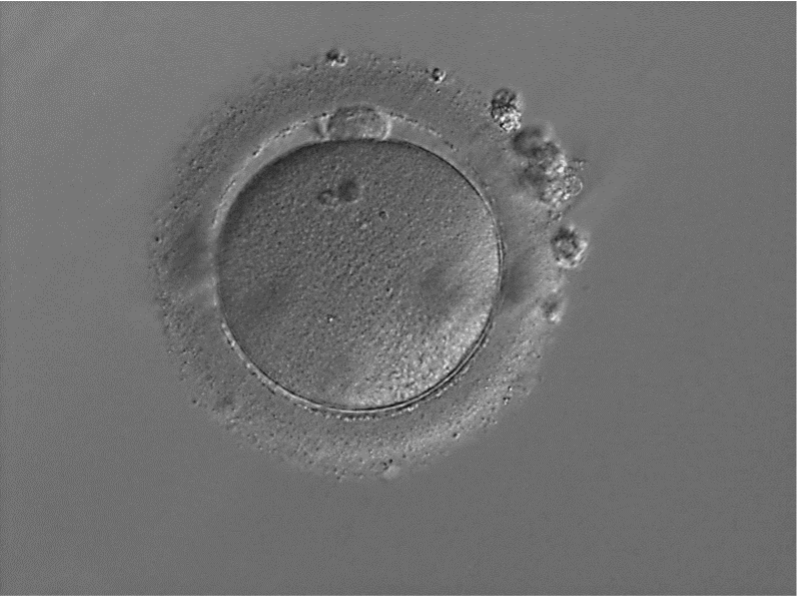
Eggs are classified as mature when a small cell (called the polar body) has been released and is visible within the shell of the egg (Figure 1).
Figure 1 – A mature egg has a small cell sitting on top of the egg known as a polar body; in this photo, the polar body can be seen at about 12 o’clock
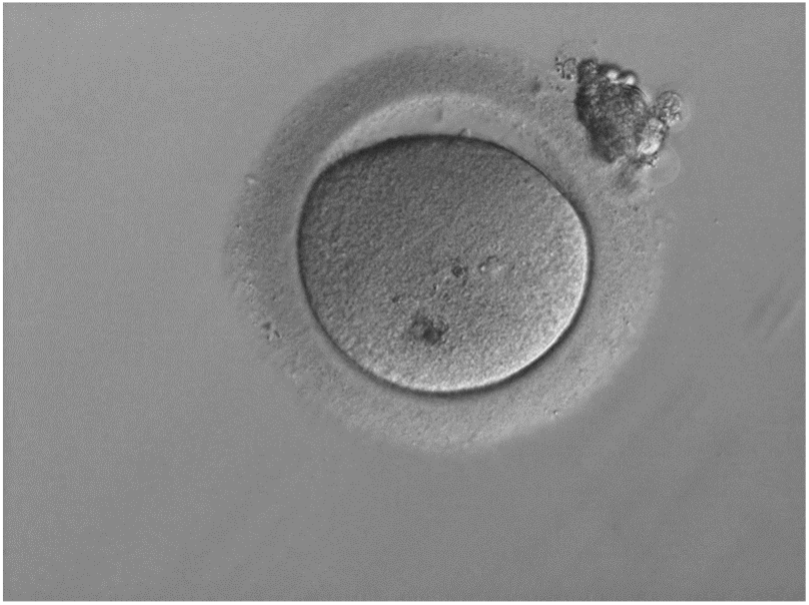
Sometimes, despite giving you hormone medication during the stimulation phase of IVF, your eggs remain immature. This occurs when maturation has started but hasn’t fully completed in time (Figure 2). These eggs may mature with time; however, when inseminated they may not fertilise at a high percentage. Unfortunately, if they don’t mature, these eggs cannot be used in the next stage of IVF (insemination).
Figure 2 – An immature egg in Metaphase I (MI) stage does not have a polar body as it has not yet been released and is not suitable for insemination
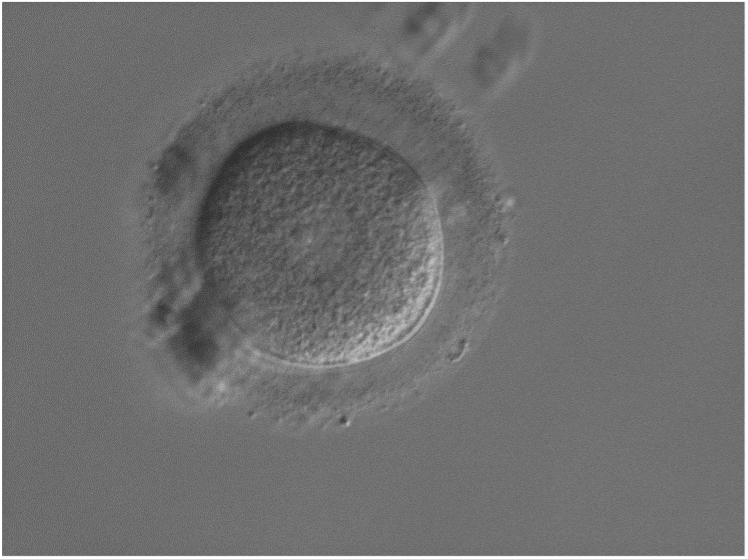
Very immature eggs (stuck at what we call the germinal vesicle stage) are distinguished by a larger, central circular nucleus (Figure 3). These eggs will not be able to fertilise and so they also can’t be used in the next stage of IVF (insemination).
Figure 3 – Very immature eggs have a circular structure in the middle called a germinal vesicle and will not fertilise
2. Insemination (bringing sperm and egg together)
In the IVF lab, there are two different methods we can use to bring your egg and sperm together:
Conventional IVF (natural insemination)
During conventional IVF, we let egg and sperm come together naturally by placing around 100,000 sperm in a special laboratory dish with 1–2 eggs we have collected and its supporting cells. Once a sperm has penetrated the egg’s supporting cells, it gains entry to the egg by sticking to, then penetrating the egg’s outer shell. In order for this to occur, both the egg and the sperm need to be mature. Mature sperm have specialised structures that allow them to successfully gain entry to an egg. While a 100,000 sperm will be placed with your egg, unfortunately, this still does not guarantee that one pair will successfully come together and fertilise.
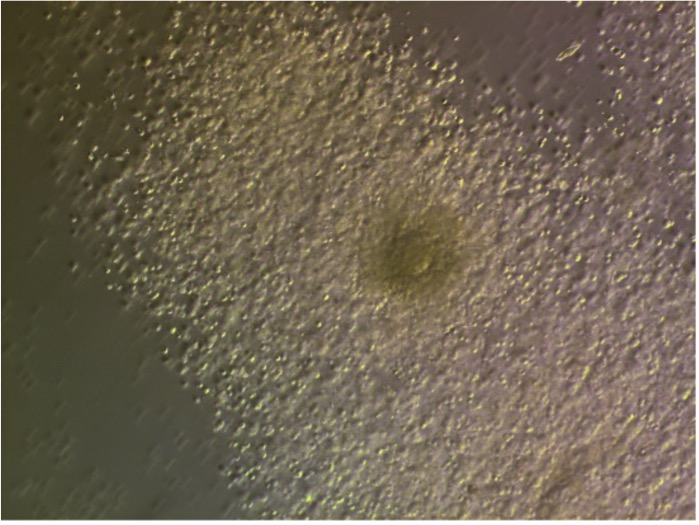
Figure 4 – An egg (the dark circular structure in the middle) with its supporting cells surrounding it (called the cumulus-oocyte complex) at the time of egg retrieval
IVF + ICSI (assisted insemination)
Sometimes during IVF we will give fertilisation an extra helping hand by using a special procedure called ICSI, instead of leaving egg and sperm to come together in a lab dish. Typically we will use ICSI when there are issues with the male partner’s sperm that preclude natural insemination in a lab dish or when conventional IVF has been attempted and was unsuccessful. ICSI stands for IntraCytoplasmic Sperm Injection and involves very precisely injecting a single, healthy sperm into a single, mature egg.
During ICSI, we first remove the supporting cells around your egg to determine if it is mature. This also helps us visualise the egg, so we can see where its DNA is. We can then position the egg appropriately so that when we introduce the sperm, we do not disrupt the DNA. Before we do this, we must also ensure that the egg’s membrane has been successfully penetrated, so that we can deposit sperm inside your egg.
When we inject a sperm into an egg, we apply gentle pressure with a special pipette (called an injection pipette), which has been pre-loaded with the sperm. Sometimes, an egg’s membrane has a lot of resistance and other times there is little or no resistance. Every now and then, the membrane of an egg may give way to the pressure of the injection pipette and break apart. If this occurs, we can no longer use this particular egg.
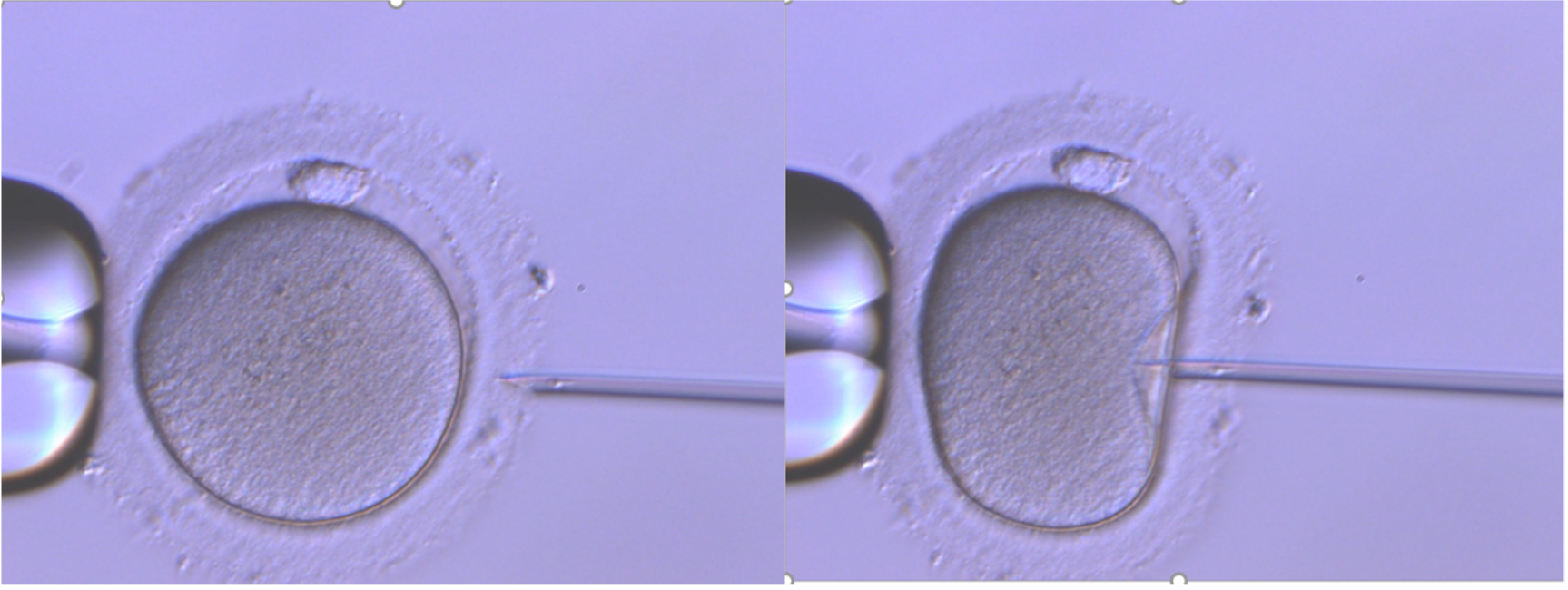
Figure 5 – A mature egg undergoing ICSI: the left image shows the holding pipette while the right image shows the injection pipette loaded with sperm
The outcomes of insemination
Normal fertilisation
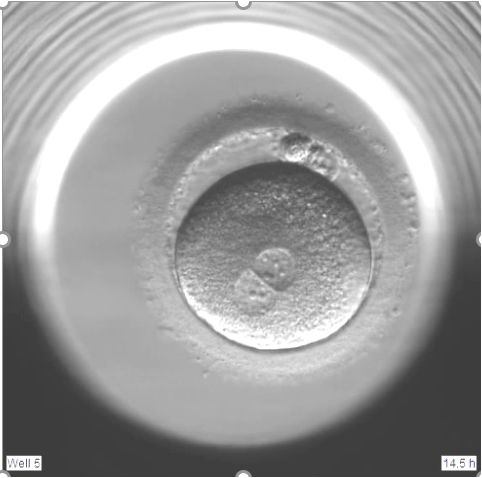
Following insemination, we can tell if a sperm has successfully fertilised an egg by looking for special structures inside the egg. In the case of normal fertilisation, we will see two distinct circles inside the egg called the pronuclei – these contain DNA from the sperm and egg (commonly referred to as 2PN, meaning two pronuclei). A second little cell (another polar body) is also released from the egg under the zona pellucida (eggshell). This can be seen the morning after insemination (day 1).
Figure 6 – Two polar bodies (about 1 o’clock) and two pronuclei (about 7 o’clock) are present, indicating that the sperm has successfully fertilised the egg
Atypical fertilisation
When an inseminated egg displays more or less than 2PN, then we classify this as atypical fertilisation.
1PN
Figure 7 – A 1PN embryo, or monopronuclear embryo, is a fertilised egg that has one pronucleus instead of two.
A 1PN is a fertilised egg that appears to have only one pronucleus. This occurs in approximately 3–5% of inseminated eggs. An inseminated egg that displays 1PN is classified as atypical.
Several factors can lead to the formation of a 1PN fertilised egg, including:
Early fusion of genetic material – The egg and sperm’s DNA may be close together, resulting in a single pronucleus surrounding both sets of DNA
Egg activation without sperm (parthenogenesis) – The egg may start developing without fertilisation. Therefore, only the egg’s DNA is present
Fertilisation with only sperm DNA – Only the sperm’s genetic material participates in fertilisation. The egg’s genetic material is not contributing, therefore preventing normal development.
These atypically fertilised embryos are less likely to develop to the blastocyst stage. However, if they progress to the blastocyst stage, genetic testing helps us determine if they have both maternal (egg) and paternal (sperm) chromosomes. Further, we can determine if these embryos can be considered for (embryo transfer).
3PN+ embryo
Figure 8 – A 3PN embryo is a fertilised egg that has three pronuclei.
In around 1–5% of inseminations, three or more pronuclei may be visible. An inseminated egg that displays 3PN or more is classified as atypical.
Several factors can lead to the formation of a 3PN fertilised egg, including:
The inability of the egg to block polyspermy: During conventional IVF, the egg’s natural defence against multiple sperm entry is not effective, allowing more than one sperm to enter the egg. This results in more than 1 set of paternal (sperm) chromosomes to be present
Abnormal egg activation: Premature/improper activation of the egg; or the second PB of the egg is not released, which can result in 2 sets of maternal (egg) chromosomes present
Sperm quality issues: Abnormal sperm may increase polyspermy risk (see point 1).
There is a high chance that these embryos are genetically abnormal and extensive genetic testing is required before considering these embryos for transfer.
With the advances in genetic testing capabilities, we can perform ‘molecular fertilisation assessments’ on embryos that have displayed atypical fertilisation and reach the blastocyst stage. This means that, with the appropriate testing, we can potentially increase the number of embryos for transfer. Embryos that do not show signs of the second polar body being released (and therefore the second set of maternal chromosomes released) would not be considered for testing as these embryos are considered abnormally fertilised.
If you are interested in testing your atypically fertilised embryos that reach the blastocyst stage please discuss this with your fertility specialist or a Newlife IVF staff member before commencing treatment. We will let you know if you have embryos that fall into this category and update you if they are developing. Please be aware there are fees involved in testing these embryos and these are per embryo and dependent on the type of testing required.
Non-fertilisation
Fertilisation is a complex process requiring precise interactions between the egg and sperm. There are several reasons why eggs may not fertilise, including:
Sperm-related functioning: Even with ICSI, some sperm may not provide the necessary signals for egg activation
Egg quality: Eggs may lack the ability to respond to a sperm’s activation signals
Lack of calcium oscillation: During normal fertilisation, sperm triggers calcium waves in the egg that initiate fertilisation and embryo development. In some cases, this process doesn’t occur as expected
Unexplained factors: Despite no obvious abnormalities, fertilisation may still not occur.
If no pronuclei are present and a second polar body has not been released, the egg has not been successfully fertilised. Alternatively, if no pronuclei are present and the second polar body has been released, this indicates that fertilisation started but did not reach completion. Once the sperm enters the egg, several reactions must occur for the fertilisation process to be successful. If components are missing from the egg or sperm or interactions are unable to occur, fertilisation will not be achieved.
Immature eggs
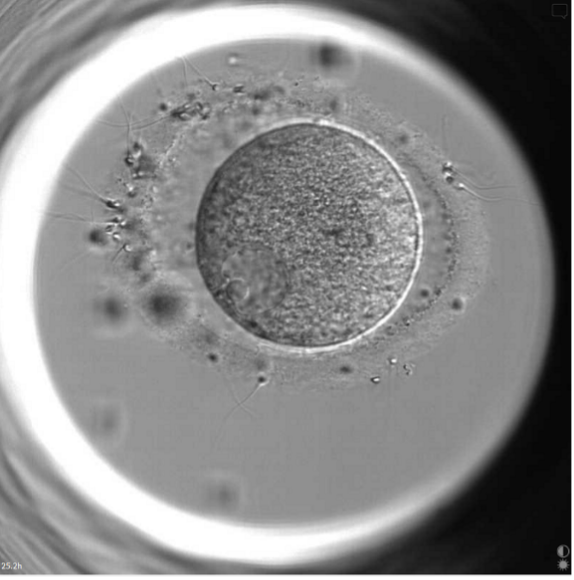
Figure 9 – An egg at the very immature germinal vesicle stage: sperm have tried to fertilise this egg (as seen by the sperm attaching to the outer shell of the egg), but because the egg is immature, sperm cannot fertilise the egg.
Unfortunately, these eggs will not form viable embryos and cannot be used in the next stage of IVF (embryo transfer).
Understanding the outcomes of fertilisation and insemination during your IVF cycle
While many different factors influence whether fertilisation during IVF is successful, having healthy, mature eggs and sperm are most critical to success. We understand every egg is precious, and we will give every egg the chance to be a viable embryo.
If you have questions at any time during your cycle, you can call (03) 8080 8933 to speak to our patient support team. They will direct you to your Newlife IVF fertility specialist, fertility nurse, fertility counsellor and/or embryologist as appropriate for the information and support you need.
Image credits: all photos shown are from the Newlife IVF laboratory.
IVF is an assisted reproductive technique that helps people overcome fertility challenges to start or grow their families. This process involves fertilising an egg with sperm in a specialised laboratory, with the resulting embryo carefully transferred into the uterus with the aim that it will lead to a pregnancy.
Whether you’re just beginning your fertility journey or considering your options, understanding the IVF process is an empowering first step. In this article, we’ll guide you through the process that we use at our fertility clinic in Melbourne, to help you make informed decisions about your next steps.
A step-by-step guide to the IVF process at Newlife IVF in Melbourne
From the initial consultation through to the embryo transfer procedure, IVF involves a series of carefully coordinated stages – tailored to your unique needs – that are designed to give you the best chance of pregnancy success.
Initial consultation with our Melbourne-based fertility specialist
If you’re concerned about your fertility and would like to seek advice from a fertility specialist, you will need a referral from your GP to attend our IVF clinic.
During your initial consultation, your fertility specialist will assess your health and the factors contributing to your fertility issues, as well as provide tailored advice, including recommendations about diet and lifestyle. This process involves taking a thorough medical history from you, performing relevant examinations and ordering appropriate tests. Your fertility specialist will also discuss all available treatment options with you so you can make an informed decision about whether the IVF process is right for you.
If it is decided that IVF treatment is appropriate, we will register you as a patient at our fertility clinic. At this stage, mandatory tests, such as screening for infectious diseases, will be conducted if they have not been done previously.
Personalised fertility treatment planning
As no two fertility journeys are the same, fertility care at our IVF clinic in Melbourne is never one-size-fits-all. Our approach begins with uncovering the root causes of your fertility challenges and guiding you through the treatment options that best suit your unique circumstances. These options can range from straightforward solutions like fertility optimisation and ovulation induction to advanced treatments, such as intrauterine insemination (IUI), IVF, or IVF with intracytoplasmic sperm injection (ICSI).
In some cases, and after a careful review of your medical and IVF history, your fertility specialist may prescribe adjuvant treatments to complement an IVF cycle.
Ovulation induction and hormone stimulation
Ovulation induction is a commonly used fertility treatment for individuals with ovulatory dysfunction. Often serving as an early intervention, it can be effective as a standalone treatment or combined with others, such as IUI or IVF, to improve the chances of conception. Ovulation induction involves using fertility medication to stimulate your ovaries to produce one or more mature eggs and assist with ovulation. For those undergoing IVF, hormone stimulation with fertility medications is used to stimulate your ovaries to produce a higher number of mature eggs than they normally would. This is a critical step in preparation for egg retrieval.
During this stimulation phase, self-administered hormonal injections are given over 8–14 days to encourage the development of multiple eggs, increasing the number available for retrieval and fertilisation.
Fertility blood tests and monitoring
Careful monitoring plays a vital role throughout the stimulation phase. Using a combination of blood tests and ultrasounds, your fertility specialist will closely track how your ovaries are responding and how the follicles (sacs in the ovaries that contain eggs) are developing. These tests allow your specialist to assess if everything is progressing as planned and fine-tune your fertility medication to optimise your results.
As you near the end of the stimulation phase, monitoring is used to determine the optimal time for the ‘trigger injection’, which prepares the eggs for ovulation (i.e. their release from the ovaries). Your fertility nurse will liaise with your fertility specialist and guide you on when to administer the injection, as precise timing is essential – the egg retrieval procedure must occur before natural ovulation. Monitoring usually takes place at one of our Newlife IVF locations in Melbourne. However, you don’t have to be in Melbourne to access treatment. We have patients that live in rural or interstate locations and we work with local pathology and ultrasound providers to assist with our patients’ monitoring needs.
Egg retrieval procedure at our IVF clinic in Melbourne
Egg retrieval, also known as egg collection or egg pickup, is a key step in the IVF process. This procedure involves collecting eggs from your ovaries, which can be frozen for future use or fertilised in the next stage of your IVF cycle.
Performed at our IVF clinic under sedation, egg retrieval is a straightforward procedure that typically takes 20–30 minutes. During this time, your fertility specialist carefully collects eggs from your ovaries using a fine needle guided by ultrasound imaging. On average, 8–12 eggs are retrieved, although the exact number depends on factors such as age, ovarian response to the medication and health history.
Collecting multiple eggs at once is important to IVF success. A higher number of eggs increases the chance of developing the healthy embryos needed for a successful embryo transfer and pregnancy.
Our team understands that undergoing egg retrieval can feel both exciting and a little nerve-wracking. But you can rest assured that we’re here to support you every step of the way so that you feel informed and comfortable throughout the entire IVF process.
Sperm collection and ICSI treatment
On the day of egg retrieval, fresh semen samples are collected from the male partner. If you’re using frozen or donor sperm, our embryologists will ensure the sample is thawed and ready for use.
For standard IVF, the semen sample is carefully prepared by removing the seminal fluid (the fluid that contains sperm), isolating the motile sperm and removing immotile sperm before the insemination procedure
For ICSI, the process is more precise. Only a single sperm is used for fertilisation, requiring experienced embryologists to select the healthiest and most viable sperm and inject it directly into the egg.
Selecting the ideal sperm is a delicate process requiring years of expertise. Our embryologists are trained to identify sperm with the best shape and structure to maximise the chances of successful fertilisation.
Fertilisation and embryo development
The next step in the IVF process is fertilisation, where egg and sperm are brought together.
In some cases, depending on the sperm quality and the patient’s previous history, we use standard insemination, where each egg is placed in a laboratory dish and exposed to thousands of prepared sperm. The fittest sperm may then fertilise the egg naturally, mirroring what would occur in the body.
However, if there are challenges such as low sperm count or abnormalities in sperm quality, an advanced technique called ICSI may be used. With ICSI treatment, a single, healthy-looking sperm is carefully injected into an egg to increase the chances of fertilisation. While this method offers additional precision, it’s important to note that not all eggs will successfully fertilise.
If fertilisation occurs, the resulting embryos are carefully placed in an incubator that mimics the conditions of the female body. Over the next five days, these embryos grow and divide, preparing for the next stage of the IVF process – embryo transfer.
The embryo transfer procedure
The embryo transfer is one of the quickest yet most important stages of the IVF process. During this procedure, a carefully selected embryo is placed into your uterus with the hope that it will successfully implant and lead to pregnancy.
Performed under ultrasound guidance, the transfer involves using a long, thin instrument to gently release the embryo through the vagina and cervix into the uterus. For most women, the procedure feels similar to a routine pap test. It is quick, requires no anaesthetic and allows you to resume your usual activities afterwards.
At Newlife IVF, our fertility specialists and embryologists are committed to providing the highest standard of care and technology to maximise your chances of IVF success.
Pregnancy testing and ongoing support
The pregnancy test represents the culmination of weeks of preparation. This fertility blood test measures the level of human chorionic gonadotrophin (hCG) in your body – a hormone produced when a fertilised egg (an embryo) implants into the uterus. Elevated hCG levels can indicate a successful IVF cycle and the achievement of pregnancy.
This test is performed approximately eleven days after the embryo transfer, giving your body the necessary time to respond to implantation. While waiting for results can be an emotional experience, our dedicated team is here to support you regardless of the outcome.
This webinar, presented by fertility specialists Dr Chris Russell and Dr Nicole Hope, provides a more detailed explanation of the IVF process.
Why choose Newlife IVF?
At Newlife IVF, we understand how significant the IVF process is, and we’re committed to walking beside you on your journey to parenthood. Whether celebrating your success or exploring the next steps, you’ll always have compassionate care and expert guidance from our team.
Clinician-owned and led fertility clinic in Melbourne
As one of few independent specialist fertility centres in Victoria, we take pride in offering a more personalised, compassionate and supportive experience compared to corporate-owned clinics.
State-of-the-art IVF treatment in Melbourne
Every aspect of our practice is thoughtfully designed with your needs in mind, from our expert-led care to our state-of-the-art laboratory and scientific tools and techniques.
Advanced scientific techniques and high IVF success rates
We incorporate cutting-edge scientific advancements into every step of our IVF treatment process, helping to give you the best possible chance of achieving a successful pregnancy.
Our approach includes the use of the EmbryoScope time-lapse system, which provides continuous monitoring of embryo development, sequential media to nurture embryos, and EmbryoGlue to enhance implantation potential when transferring embryos into the uterus.
For ICSI treatment, we take it a step further with egg spindle visualisation technology, allowing us to carefully select eggs with the greatest potential for fertilisation.
Our IVF success rates reflect the effectiveness of these methods, consistently exceeding the national average and giving our patients a better chance of achieving their dream of parenthood.
Accessible and affordable IVF treatment in Melbourne
At Newlife IVF, we believe that everyone deserves the opportunity to build their family, which is why we are committed to providing affordable IVF treatment. Our fee structure is designed to be transparent and accessible, ensuring that fertility care in Melbourne, including IVF, is reasonably priced and doesn’t involve the stress of unexpected costs.
Contact Newlife IVF – your trusted fertility clinic in Melbourne
Babies are in this embryonic stage until week 9 of pregnancy, after which we use the term foetus. The ability to grow embryos in a laboratory environment (outside the woman’s reproductive tract) was a huge scientific achievement. This led to the development of in vitro fertilisation (IVF) as a way of helping couples fall pregnant if they could not do so naturally.
While you can’t always see what embryologists do during your IVF journey, their care of your eggs, sperm and embryos plays a huge part in the success of your treatment. As Chief Embryologist and Scientific Director at Newlife IVF, I oversee our amazing team of embryologists and ensure our laboratory is set up according to best scientific practice. In this article, I explain a little bit about what we do ‘behind the scenes’ in order to help women and couples conceive.
What role does an embryologist play during fertility treatment?
The laboratory is often referred to as a fertility clinic’s ‘engine room’. This is where our embryologists manage many of the steps involved in IVF. Our role in the IVF process usually begins during the egg retrieval stage. Under a microscope, we carefully examine the fluid your doctor collects from the mature follicles inside your ovary. We identify and extract any healthy eggs we find, before placing them in a laboratory dish with a specially prepared sample of your partner’s sperm (or donor sperm, if required). We then ‘keep watch’, checking for signs of fertilisation (when egg and sperm unite to form an embryo) and monitoring the growth of any embryos that do develop. In some cases, we will inject a single sperm directly into the woman’s egg to increase the chances of fertilisation. This technique is called intracytoplasmic sperm injection (ICSI).
Embryologists are also responsible for freezing and storing embryos. A woman may need to freeze and store her embryos if she has opted for a frozen embryo transfer (rather than a fresh embryo transfer) and/or if she has multiple embryos following egg collection and insemination. Only one embryo is transferred into the womb at a time, so we freeze any extra embryos in case implantation fails and repeat embryo transfers are required in the future. We store embryos at sub-zero temperatures using a process called cryopreservation.
Beyond IVF, we also freeze and store eggs for women who choose to freeze their eggs as a way of preserving their future fertility. We can even freeze sperm. This is actually incredibly important, as it allows us to maintain a bank of donor sperm for single women and couples (including lesbian couples) who rely on sperm donation to start their families.
How do embryologists help ensure a healthy baby?
There are a number of measures we employ in the laboratory to ensure patients are given the best chance of having a healthy baby. First and foremost, our in-house laboratory was specially designed to reduce volatile organic compounds (VOCs) and harmful blue light, ensuring optimal conditions for embryo development. Day-to-day, we also adhere to strict quality-control protocols, which are designed to maintain ideal conditions within the laboratory environment for embryo growth.
Our embryologists also use extra lab procedures that not all fertility clinics offer. We routinely use these techniques as part of our standard practice to optimise embryo development and give your embryo the best chance of successfully implanting in the womb. This includes the use of the EmbryoScope time-lapse system, sequential media and EmbryoGlue.
In some cases, we will employ even more specialised techniques to help us assess your eggs, sperm and embryos, so that we can select the best ones to use during IVF. This includes preimplantation genetic testing (PGT) of embryos. By carefully removing a small number of cells from a developing embryo, we can determine if the embryo is carrying a genetic disease (PGT-M), has the right number of chromosomes (PGT-A) or changes in the size or arrangement of chromosomes (PGT-SR). These tests require a highly experienced embryologist with special skills, so they are not offered by every fertility clinic. While PGT is not suitable for everyone, it can help lead to successful pregnancy in certain couples, such as those with a history of recurrent miscarriage or repeated unsuccessful IVF cycles. Your fertility specialist can advise if PGT is right for you.
In the case of ICSI, our embryologists use microscopes connected to micromanipulation equipment (e.g. micropipettes) to select individual sperm and inject this directly into the woman’s egg. Sometimes, we may use another technique if necessary, called intracytoplasmic morphologically selected sperm injection (IMSI), to help us pick out a healthier sperm based on its shape. We also use polarised light microscopy to assess a structure inside the egg called a ‘spindle’. We call this ‘egg spindle visualisation’. This allows us to identify if an egg is at a certain stage of development (called metaphase II) and therefore, in optimal condition for fertilisation via ICSI treatment.
Each of these lab processes requires exquisite attention to detail, extreme care and exhaustive consideration of multiple variables that can affect the healthy growth and development of embryos, as well as the ‘well-being’ of your eggs and sperm.
Is there a ‘typical workday’ for an embryologist?
No two days are ever the same! Every case is unique — whether we are caring for sperm, eggs, embryos or patients. There are always different challenges to manage or breakthroughs to celebrate. We are constantly amazed by the potential of these tiny-celled structures. And, of course, ongoing advances in the science behind IVF means that we are also continually learning new skills and adapting to new technology as well.
What level of involvement does an embryologist have with patients?
Patients typically get very little exposure to what is going on behind a lab’s doors. Understandably, this can make IVF even more daunting for patients. That’s why, at Newlife IVF, our embryologists make a point of staying in close contact with patients throughout their fertility journey. We are very mindful of the fact that patients have entrusted us with their future, and that their eggs, sperm and embryos are incredibly precious to them. Our embryologists are always available to speak to patients and answer their questions. Our goal is to keep patients well informed at all times about the status of their embryos and how everything is proceeding in the lab, so that they feel reassured that their embryos are being properly cared for.
What is the best part about being an embryologist?
Being able to help couples achieve what they want most in the world is extremely rewarding. It’s incredible to be able to watch a life begin under the microscope and emerge months later as a healthy baby. Embryology is a fascinating field that is constantly evolving, and I feel a great sense of pride at being part of such a life-changing science.
Ready to start your fertility journey?
At Newlife IVF, you can rest assured that an experienced embryologist will be part of your fertility team. You can visit our team page to read more about Dr Tiki Osianlis and some of the other embryologists at Newlife IVF. If you’re ready to take the next step in your fertility journey, you can start today by making an appointment with one of our fertility specialists — call (03) 8080 8933 or book online.
As science and technology have progressed, so too have the techniques we can use during embryo transfer to increase the chances of a successful pregnancy. Below we outline the specific techniques we use at Newlife IVF to facilitate success during this part of the IVF cycle.
1. Growing and selecting the best embryo
During IVF, your eggs, sperm, and later embryos, are kept in an incubator. An incubator is a bit like an oven. It maintains a stable environment (including an even temperature), which helps the embryos to grow and develop.
As your embryos grow in the incubator, we observe them very carefully. In the past, this meant repeatedly opening the incubator at regular intervals to get ‘snapshots’ of their growth – but this also meant that we were constantly disturbing the embryos as they developed.
More recently, advances in technology have led to the development of a special type of incubator called the EmbryoScope time-lapse system. The EmbryoScope has a built-in camera and high-powered microscope, which enables us to automatically capture images of your growing embryos every 10 minutes. Essentially, this means we no longer have to keep opening the ‘oven door’, allowing us to closely monitor the development of your embryos without disturbing them.
The benefits of this are two-fold:
We ensure a stable environment for embryo growth, which contributes to embryo quality, and;
We get a more complete picture of embryo quality, enabling us to select the best embryo for transfer.
In most cases, we will select embryos that are at the ‘blastocyst’ stage of development (around 5 days old). This is roughly the same time that an embryo would normally be in the uterus after a natural conception. Transferring the embryo at this stage (instead of the earlier ‘cleavage’ stage around day 2–4) means the embryo is more mature and has already demonstrated its potential for strong growth. Blastocyst transfer may also reduce the risk of the embryo being expelled from the mother due to altered levels of hormones that can occur after the egg freezing process.
The other benefit of waiting until embryos have reached the day 5–6 cell stage is that we can test them for chromosomal or specific genetic defects prior to transfer using preimplantation genetic testing. These tests are not recommended for everybody but may be advised if you are older, have experienced recurrent miscarriage or multiple failed IVF cycles. In this case, our aim is to screen out any embryos with genetic anomalies that are unlikely to result in an ongoing healthy pregnancy, so that the embryo with the best potential for development can be placed in the womb.
At Newlife IVF, we routinely use the EmbryoScope time-lapse system for all IVF procedures, as part of our standard of care. Patients do not pay more for this technology. It is included in our standard cycle fees.
2. Deciding the optimum number of embryos to transfer
In the past, it was common practice to place two or more embryos in the womb at the same time, with the aim of increasing the chance of success. However, this practice has fallen out of favour due to the likelihood of a multiple pregnancy (e.g. twins or triplets). While this may seem like an ideal way to complete your family in one go, multiple pregnancies actually carry an increased risk of miscarriage and other complications. For this reason, our preferred practice at Newlife IVF is to transfer a single, high-quality embryo. That’s why we put a lot of effort into selecting the right embryo to transfer.
3. Guiding and protecting the embryo during transfer
The way an embryo is transferred into the womb is also critical to its success. We use a thin, flexible tube, called a soft catheter, to guide the embryo and protect it during its journey from the incubator to the womb.
For the best possible odds of an ongoing pregnancy, the embryo also needs to be placed in the correct location within the womb. Every woman’s uterus can vary in shape, so we may sometimes conduct a ‘mock embryo transfer’ before the actual procedure to determine the location and transfer technique that will give the best chance of success.
During the transfer, we use ultrasound imaging (the same technology used to view a baby in the womb) to provide us with real-time information about the catheter’s location, enabling highly accurate placement of the embryo in the womb.
4. Helping the embryo to implant in the wall of the womb
Once the embryo has been placed in your womb, it must attach to the wall of the uterus in a process called implantation before it becomes a viable pregnancy.
To improve the likelihood that the embryo implants, we place the embryo in a special substance called EmbryoGlue before we transfer it. EmbryoGlue was developed following the discovery that certain compounds that occur naturally in the body may help the embryo attach to the wall of the uterus.
A major component of EmbryoGlue, hyaluronan, is normally found in the uterus and has chemical properties that increase cell viscosity. This is thought to assist the embryo to attach to the wall of the womb, increasing the chances of implantation and a successful pregnancy.
Fresh versus frozen embryo transfers
Using fresh or frozen embryos affects the timing of your embryo transfer. In a fresh transfer, the embryo is transferred 3–5 days after egg collection and fertilisation (once it has reached the blastocyst stage). In a frozen transfer, previously frozen embryos are thawed and transferred into the uterus at a later date.
While many assume that a fresh embryo transfer is faster or more effective, this is not always true. During IVF, hormone levels can rise significantly, which may prime the uterus to become receptive to implantation before the embryo has reached the necessary blastocyst stage. The use of frozen embryos allows us to avoid this issue. Freezing embryos shortly after they reach the blastocyst stage provides additional time for hormone levels to return to their normal cyclical rhythm, allowing us to align the window of uterine receptivity with the embryo transfer.
Frozen embryo transfer may also be more suited to patients who have high progesterone levels at the time of egg collection, those with PCOS, or anyone undergoing genetic testing of embryos, which requires additional time. Comparably, fresh transfer may be suitable for patients with a limited number of embryos or where time-to-pregnancy is a consideration.
At Newlife IVF, your fertility specialist will help determine the most suitable approach based on your unique circumstances to improve your chances of a successful embryo transfer.
What to expect on the day of your embryo transfer
An embryo transfer is a straightforward procedure. The experience is comparable to a Pap smear, and an anaesthetic is not needed. Most women can return to their usual activities shortly after the procedure.
We aim to optimise every step in the treatment cycle
By employing advanced scientific techniques like these at every step in the IVF cycle, we aim to give our patients a better chance of achieving a successful pregnancy sooner.
If you would like advice specific to your circumstances or a second opinion, you can make an appointment with one of our fertility specialists by calling Newlife IVF on (03) 8080 8933 or by booking online. This appointment does not need to be about IVF specifically – there are many different ways we can assist with conception depending on your fertility needs.
Once here, it must ‘implant’ in the wall of the womb and grow before we can say that IVF has resulted in a successful pregnancy. The timing of embryo transfer can vary, depending on whether the embryos being transferred are ‘fresh’ or ‘frozen’. Fresh embryo transfer refers to embryos that are transferred to the uterus 3–5 days after a woman’s eggs have been collected and fertilised by sperm. Frozen embryo transfer refers to embryos that have first been frozen before being thawed at a later date for transfer into the womb.
In the early days of IVF, fresh embryo transfer was the favoured approach. However, the techniques used for freezing and thawing of embryos have since improved to a point where more than 90% of embryos will survive the process. Consequently, a ‘freeze-all’ strategy has become more common, whereby all embryos are frozen following successful growth. They generally remain frozen for at least a month before the best embryos are thawed and transferred into the womb.
Understandably, people undergoing IVF are often eager to get pregnant as quickly as possible – and may assume that fresh embryo transfer is both faster and more effective. But is one approach better than the other?
To appreciate the pros and cons of fresh versus frozen embryo transfer, you first need to understand the so-called ‘window of uterine receptivity’.
The window of uterine receptivity
The success of embryo transfer depends on a number of factors, one of which is uterine receptivity – that is, how ready the uterus is to ‘receive’ the embryo. Outside this window of receptivity, the embryo may fail to implant in the wall of the uterus.
To receive the embryo successfully, the uterus must be ‘primed’ by the hormones oestrogen and progesterone. Under natural conditions, the priming of the uterus is perfectly timed with a woman’s monthly cycle, such that if an egg is released from the ovary and fertilised by sperm, the uterus is ready to receive the embryo. In the IVF setting, however, this timing may be less than perfect.
During IVF, the ovaries are stimulated via self-injectable medication so that the highest possible number of eggs can be collected. By artificially driving the release of so many eggs, the levels of oestrogen and progesterone skyrocket – they can rise to 10 times higher than normal peak levels. This may cause the uterus to prematurely prepare itself for embryo implantation, bringing forward the time frame in which the uterus is receptive. The problem with this is that by the time a fresh embryo is grown and ready for transfer, the window of uterine receptivity may have passed.
Frozen embryo transfer overcomes this problem by delaying the transfer process. This gives the hormone levels time to return to normal and the embryo is then transferred at a later date, when the uterus is receptive again.
When is frozen transfer best?
There are some situations where frozen embryo transfer may be considered the best option, including:
High levels of progesterone: When progesterone levels are high at the time of egg retrieval, there is a higher chance that the window of uterine receptivity will shift forward. In these cases, it is generally better to freeze the embryos and transfer them later when the uterus is receptive again.
Polycystic ovary syndrome (PCOS): Studies have found that women with PCOS tend to have better results from frozen versus fresh transfer. Frozen transfer reduces the risk of ovarian hyperstimulation syndrome (a complication of egg retrieval), and is also associated with a higher chance of ongoing pregnancy.
Embryos that require genetic testing: The genetic testing of embryos takes time. Consequently, by the time a tested embryo is ready for transfer, the window of uterine receptivity is likely to be over. In this scenario, frozen embryo transfer is usually more appropriate.
What are the arguments for fresh transfer?
On the other side of the coin, fresh transfer avoids the need for the freeze-thaw process. While current technology enables a greater than 90% survival rate for frozen embryos, this level of risk may not be acceptable for some patients – especially if they already have a low number of embryos. Fresh transfer potentially also results in a shorter time to pregnancy.
Which is the best option for you?
When choosing between fresh and frozen embryo transfer, there is no one-size-fits-all approach. As with all aspects of fertility care, the decisions need to be personalised to your individual circumstances. Our fertility specialists will assess the specifics of your situation and tailor their advice accordingly.
If you would like professional advice about the next steps to take on your fertility journey, you can make an appointment with one of our fertility specialists by calling Newlife IVF on (03) 8080 8933. Alternatively, you can book online via our appointments page.
To help avoid this confusion and facilitate communication between fertility specialists, researchers and patients, a group of reproductive health organisations developed a standardised glossary of fertility-related terms and definitions.
This glossary includes recommendations for the terminology used to describe genetic testing of embryos. Previously referred to as PGS (preimplantation genetic screening) and PGD (preimplantation genetic diagnosis), all genetic testing on embryos is now known as PGT (preimplantation genetic testing).
The different types of genetic testing are differentiated by the addition of further letters to the PGT acronym: namely PGT-A, PGT-M and PGT-SR. To understand the meaning of these terms and the types of genetic testing they refer to, it first helps to understand some basics of genetics.
A brief lesson on genetics
You may have heard of the term ‘chromosome’ before. Chromosomes are structures that house our DNA, which is the genetic code that contains all the instructions required to make you, you! Normally, every cell in the body contains 46 chromosomes. These chromosomes are inherited – during fertilisation (when egg meets sperm), 23 chromosomes are passed on from each parent.
There are many different types of genetic errors that can occur, and a wide range of genetic conditions they can give rise to. One type of error is an abnormality in the number of chromosomes, which is referred to as aneuploidy. Instead of 46 chromosomes, a person may have 45 or 47 chromosomes, as seen in Turner and Down syndrome, respectively. Embryos that have an abnormal number of chromosomes are less likely to result in an ongoing pregnancy.
Small errors may also occur in the DNA contained within the chromosomes. These errors are known as genetic mutations and can give rise to diseases such as cystic fibrosis and haemophilia.
Lastly, errors can occur in the structure of the chromosomes, including changes to their size or how the DNA is arranged within them. This is not the same as aneuploidy – many people with structural rearrangements have a normal amount of DNA overall. If that is the case, the person will probably not be affected by the rearrangement. However, someone with a structural rearrangement has an increased risk of producing an embryo with an abnormal amount of genetic material, which is less likely to result in a healthy, ongoing pregnancy.
The different types of genetic testing
There are three different types of genetic testing that may be performed on embryos:
PGT-A (preimplantation genetic testing for aneuploidies): PGT-A used to be known as PGS. It is designed to identify the embryos that have an abnormal number of chromosomes (aneuploid embryos), as these embryos are less likely to result in an ongoing healthy pregnancy.
PGT-M (preimplantation genetic testing for monogenic or single gene defects): PGT-M was previously known as PGD. PGT-M assesses the embryo’s genetic code to determine if it contains mutations that may result in certain genetic conditions, such as cystic fibrosis or haemophilia.
PGT-SR (preimplantation genetic testing for chromosomal structural rearrangements): Like PGT-M, PGT-SR was also previously known as PGD. PGT-SR detects structural rearrangements in an embryo’s DNA and can detect whether the embryo has the correct amount of genetic material.
How do you know if genetic testing is appropriate for you?
Not all patients require PGT, and each type of PGT is only appropriate for particular groups of people. Your Newlife IVF fertility specialist can advise whether genetic testing is suitable for you. To make an appointment, call (03) 8080 8933 or book online via our appointments page.